Systemic detox
Inventory and critical evaluation of current detoxification methods and remedies
At no time in its history has mankind been exposed to a comparable toxic burden as today. Year after year, industrial production releases millions and millions of tons of synthetically produced pollutants and toxic compounds into the environment – not only in the context of such catastrophes as we have just experienced again in Japan. There is a method to this madness! It is part of our canon of values: unlimited feasibility combined with unlimited greed for pecuniary values.
Basics: Bioaccumulation, barrier systems and biotransformation
At no time in its history has mankind been exposed to a comparable toxic burden as today. Year after year, industrial production releases millions and millions of tons of synthetically produced pollutants and toxic compounds into the environment – not only in the context of such catastrophes as we have just experienced again in Japan. There is a method to this madness! It is part of our canon of values: unlimited feasibility combined with unlimited greed for pecuniary values.
Among the more massive environmental burdens of recent times are even well-intentioned, but basically more than aggravating attempts by our ecological saviours, as we are experiencing in the reduction of exhaust pollution by fine dust filters in diesel engines. While our immune system with its macrophages was still somewhat equipped against the large particles from fat-containing soot, our lungs are helplessly at the mercy of the eco-fine dust and its nanoparticles from the new filters. The increase in lung diseases speaks for itself.
There are countless such toxic sites, from amalgam to mercury-containing energy-saving light bulbs to the biophenols in plastic bottles. In Germany alone, 30,000 tonnes of pesticides are applied per year. This is a comparatively small amount compared to countries like Spain, where tomatoes and the environment in the Guadálquivir river delta are deliberately poisoned to end up on our plates as “sun-ripened” vegetables. Not to mention the Third World countries in Africa and Asia to whom we sell our efficient industrial poisons when their use is banned at home. A simple head of lettuce is sprayed with pesticides a staggering 15 times before it is harvested. The load of one kilogram of conventionally grown carrots may contain 5,000 mg of pesticides for “adults” over three years of age, while the same carrot may not exceed 10 mg per kilo according to baby standards with intake until the age of three. A Lake Constance apple is maltreated with up to 28 different pesticides in order not to exceed the maximum permissible values for individual substances. And German winegrowers are suddenly discovering organic, supposedly because such wines are healthier. In reality, the “discovery of organic” under the guise of quality is about countering the stifling competition from third countries with new marketing measures – fortunately, one must say, the competition is stifling.
The very term conventional agriculture is a euphemism of the first order.
The destruction of soil structure, soil life and the ecological biodiversity of micro- and macro-organisms form its basis. 150 years of chemical-industrial madness are sold as normality, while more than 10,000 years of agriculture in harmony with nature are considered inferior.
One of my Parkinson’s patients, when asked specifically and after testing an enormous pesticide load with a bioenergetic analysis, told me that he was the son of a winegrower and that in his early youth he had often applied large amounts of pesticides with his tractor. Each time, he would have come back completely soaked to the skin from the spray clouds of synthetic poisons. He probably would not have thought of wearing a protective suit. Another patient with severe CNS poisoning told me similar things after the test. He had a 30-50 cm tremor in his right arm and extreme stiffening of the thigh muscles due to years of trembling. He had been undergoing various unsuccessful attempts at diagnosis and treatment for about three years, until in the end he was diagnosed with a neurological problem and recommended further medication in addition to the existing intoxication. By the way, he was a hazardous goods manager for a large chemical company. With the help of my special metabolic programme, targeted detoxification and the use of microcurrent therapy, he was almost completely tremor-free within 3 months, the hardening of the thighs had disappeared and the muscles were soft again.
1.1 Bioaccumulation
Many plants also produce toxic, secondary plant substances as a defence against enemies. And finally, microorganisms such as moulds also secrete toxins that have a more or less strong toxic effect on the mammalian organism. It is not always exogenous moulds such as Aspergillus flavus with its aflatoxins or Aspergillus fumigatus, which we inhale in large quantities near compost heaps, for example. Günther Enderlein already pointed out more than 80 years ago that fungal forms living symbiotically with us, such as Mucor racemosus and Aspergillus niger, strive to create their own environment. They produce organic acids and are enzymatically active. Thus, Mucor racemosus synthesises lactic acid and Aspergillus niger citric acid, but also calcium, which is deposited as complexed calcium, i.e. calcium bound to bicarbonate, phosphate or lactate or to albumin, and is not bioavailable like ionised calcium. As a result, hypercalcaemia and hypocalcaemia may well occur side by side. The accumulation of organic acids and enzymes by these symbionts can lead to metabolic derailment of the host and cause severe health damage. Multicellular parasites such as roundworms and flatworms, etc. with their high affinity for toxins and heavy metals, which themselves also secrete toxic metabolic degradation products and whose effects are then often declared as food allergies, are also often overlooked.
Humans are at the top of the food chain.
Through bioaccumulation, pesticide contamination can accumulate in plants over several stages. From herbivores, which eat the plants, to carnivores, which eat the herbivores, the path runs all the way to omnivorous humans, where the toxins can concentrate thousands, even millions of times over. Of course, this also applies to other animals at the top of the food chain. For example, the thin eggshells of the white-tailed eagle are an expression of the increased intake of toxins by fish swimming in the toxic waste of our rubbish. In children, we then experience behavioural disorders after multiple inoculations, such as ADHD with or without hyperactivity – “fidgeting” or autistic rigid. In adult men, azoospermia and infertility in women are becoming more frequent.
So today we do not necessarily need the more subtle forms of intoxication with which modern medicine delights us, such as mercury-containing vaccines, dental amalgam or medicines. The daily intake of environmental toxins through breathing, drinking and eating alone has reached frightening proportions. Electrosmog, systemically amplified by the accumulation of heavy metals that amplify the signals like antennae in our bodies, adds to the problem. But the overload of toxins does not seem to be enough. Stress, lack of exercise, malnutrition, bad water or even a life of soft drink intoxication create a “carcinogenic” lifestyle. Together with the destruction of the biological basis of our food, this reduces the power of our organism to maintain its daily detoxification work. Fibre intake alone, which contributes to daily intestinal detoxification, has decreased by 90% compared to a rural man of just 60 years ago.
All these factors widen the gap between daily intoxication and daily detoxification capacity of our body, resulting in enormous cumulative processes over the years. The insidious results of such accumulations over years and decades can be chronic, chronic-degenerative and multisystemic diseases with mitochondriopathies. Often, however, these clinical pictures are not even remotely associated with the problem of creeping intoxication and an increasingly disturbed detoxification capacity, but are usually interpreted as age-related or inherited. But one should know better. This knowledge is used in the targeted killing of rats, which are given poisoned food that only shows its effects weeks later and is not recognised by the animals. The highly intelligent animals would immediately pass on the death by life-threatening food as information to the following generations, which they cannot do, however, because they cannot immediately recognise the connection between food intake and their death caused by it. Just like us humans. Incidentally, rats prefer organic food, as laboratory experiments have shown. The result: fewer stillbirths than when fed products from “conventional” cultivation.
With regard to their own health, people do not seem to be aware of the consequences of such creeping poisoning, although long-term damage caused by toxins in diseases such as cancer, Alzheimer’s or multiple sclerosis has long been the focus of many scientists. One of the reasons for the lax handling of these things is certainly the ability of our body to adequately compensate metabolically for such systemic stresses over many years and decades.
1.2. Hydrophilic and lipophilic toxins, exposure to radiation
to cope with environmental toxins, but it has difficulty disposing of many of the synthetic toxins. The residence time and hazardousness of toxic substances in a biological system are strongly determined by their chemical and physical properties. If a compound is water-soluble, it can usually be metabolised and excreted quickly because our organism has a wide range of enzymes available for this purpose, which can also break down complex molecules. The basic prerequisite for this is first of all, of course, the sufficient consumption of detoxification-supporting nutrients and the solvent required for this: water in an energy-rich, ionised form. However, the high metabolisation capacity does not apply to all water-soluble toxins. Some of them are incorporated into the body’s own tissues to mitigate their immediate toxicity and are deposited if the body fails to excrete them in time. These include lead, for example, which, when deposited, can occupy the junction sites of iron in the blood or calcium in the bones because it has similar atomic radiants.
Beethoven is a tragic example of this. For a long time it was assumed that he, as a passionate wine drinker, was so highly contaminated with this heavy metal because of the lead salt content in the wine to bind the tartaric acid. In the meantime, it has been discovered that it was state of the art in orthodox medicine at the time to administer lead salt for pneumonia, among other things. When Beethoven developed ascites in response to his doctor’s initial treatment, it had to be punctured. To make matters worse, the attending physician then again used a wound ointment containing lead salts. The skull fragments that were discovered a few years ago in the USA and examined for their authenticity still show a lead contamination 200 times higher than the norm.
As a hydrophilic substance, lead cannot pass the blood-brain barrier. Nevertheless, the high blood circulation in the circumventricular space of our brain of up to 900 litres of flow per day (= 13 % of the cardiac output) automatically causes a higher “turnover rate” in an adult on average, so that an increased storage of lead in the calvaria of the skull is not surprising, if only because of the frequency of passage. Other famous men, such as the Spanish painter Franzisco Goya, who died after a serious illness and mental confusion, were also severely poisoned by the lead-containing paints that we still import from the Far East in children’s toys. Scientists suspect that his sperm were also enormously contaminated and that this caused his wife’s 16 miscarriages.
The situation is much more problematic with lipophilic toxins. These include the pesticides and herbicides already mentioned, but also solvents, plasticisers and nicotine from tobacco consumption and – not to be forgotten – the organic mercury compounds that we would like to be administered collectively in vaccinations. Not only are they metabolised more slowly than their hydrophilic counterparts, they are also more easily deposited due to their fat-binding ability and can be successfully accumulated in fatty tissue, which is definitely a certain “richness” given the increasing obesity of our population. This bioaccumulation has fatal consequences in the long run. By depositing, for example, on the transport systems of the various compartments, they can considerably impair the active and passive transport of substances of the intermediary metabolism. By blocking channel proteins of the cell, they prevent the passive process of facilitated diffusion, which prevents the supply of nutrients to the cell, but also the removal of toxins from the cell. Active transport between the mitochondrial matrix, mitochondrial membrane and cytoplasm via carrier systems or substrate chain phosphorylation to generate the charge gradient-dependent chemo-osmotic coupling can also be disrupted. Heavy metals reduce or increase the charge potential of the cell membranes through their electro-chemical effect and thus interrupt the so important biochemical cascade of the citrate cycle and cell respiration. Radioactive radiation also interferes with metabolic processes, e.g. via the thyroid gland. As therapists, we refer to this in somewhat simplified terms as blockages. Mercury, for example, docks onto important binding sites of molecular compounds with thiol or hydroxyl groups and in this way can block important enzymatic reaction steps such as methionine or glutathione biosynthesis. Glutathione is one of the cell’s most important antioxidants. The result can be extensive damage to the mitochondria, thus promoting the development of mitochondriopathies and multisystemic diseases.
1.3. Barrier systems, levels of detoxification and biotransformation
In order to better understand these processes, we cannot avoid some basics of biochemistry that are important for detoxification. In my opinion, most mistakes in the detoxification and elimination of toxins arise from ignorance of the different biochemical processes in the respective reaction spaces, at least as far as they are known to date.
For my further argumentation, I will first distinguish between three major barrier systems and the three detoxification levels of the human organism resulting from this classification. Nutrients and substrates from the food supply and the intermediate metabolism, as well as toxins, must in principle overcome all three large barrier systems in the human organism in order to reach the organ-specific cell and cell subsystems, so that an analogous division of detoxification and recycling at these three levels is appropriate.
Finally, there is the process sequence itself, which can be roughly described as a three-stage cascade of biotransformation of toxins in mammalian biological systems.
1.3.1. The different barrier systemse
The second major barrier system consists of the transit route between the bloodstream and the parenchyma, including the transition via the membrane systems of the cell and organelles into their subsystems. I thus combine bloodstream pathways, extracellular space (EZR), intracellular space (IZR) and the matrix of organelles into one barrier unit.
I only differentiate this second barrier system from the brain, which has developed a third barrier system consisting of the blood-liquor barrier (BLS) and the blood-brain barrier (BBB), which occupies a special position.
All barrier systems in turn have a multi-level structure and can be compared to the different access levels of a dam and sluice system.
The first protective film in the first large barrier system is formed by the mucus-water layer in the intestine, in whose ecosystem billions of symbiotic bacteria build up a second passive protective layer. The intestinal mucosa itself forms the next level of protection with a huge contact surface of up to 400 m2 through the so-called tight junctions. It marks the regulated “border crossing” between the outside world and the bloodstream. Following this, a fourth barrier is built up with the intestinal immune system as part of the mucosa-associated lymphatic tissue, before it passes into the portal vein, which with the liver represents a further boundary point. Toxins that have managed to cross the intestinal or mucosal barrier (GALT as Gut Associated Lymphoid Tissue and MALT as Mucosal Associated Lymphoid Tissue) and flow to the liver via the portal vein can be conjugated and degraded there if the nutrient situation and detoxification powers of the liver are sufficient.
An intact physiological intestinal flora, a sufficient supply of nutrients and a functioning liver are therefore the most important basic prerequisites of any successful detoxification.
large barrier system in the intestine, for example due to a leaky gut syndrome, must be excluded before a detoxification measure, as otherwise intestinal reabsorption of highly toxic metobolites can occur. I refer to this level of detoxification as “the detoxification of the extreme within”. Even the crossing of this barrier by allergenic proteins – for example in leaky gut – causes a kind of “detoxification action” through a GALT- and MALT-associated antigen-antibody reaction (AAR).
The second barrier stage extends from the bloodstream via the transit route of the Pischinger space to the parenchyma and, in my definition, also includes the passage into the compartments of the cell and its subsystems. Here, as already in the mucosa-associated tissues, further defences are controlled by appropriate antigen-antibody reactions, pH-milieu regulations and the barriers of the membrane systems of cells and organelles. I refer to this level of detoxification as “the detoxification of the inside within”.
Finally, we have the brain with its special position. With just 2% of the body mass, it still consumes 20% of the total energy. In one minute, 610 ml pulsate through its capillaries; extrapolated over 24 hours, that makes about 900 litres. It reacts much more sensitively than other organs to fluctuations in the oxygen content, to the deprivation of nutrients or to exposure to toxins. Maintaining its stable equilibrium is therefore a top priority. In order to ensure this, it has developed a sophisticated, two-stage barrier system, which in turn has several levels: the more functionally oriented blood-liquor barrier (BLS) and the functional and physiological barrier of the blood-brain barrier (BBB). Behind this graduated system of “barriers” in both directions lies a complex regulation that is linked to each other via a network of tissues with different morphological structures. It is intended to ensure optimal supply with the best possible demarcation and to guarantee the exchange of substances flowing in both directions.
The endothelial tissue of the brain capillaries shows structural similarities with the construction principles of other tissues, especially those of the intestine, with which it shares developmental parallels. In humans, for example, the intestine has regressed reciprocally and proportionally to the growth in size of the brain. Brain and intestine as so-called expensive tissues therefore not only share many neurotransmitters, which is why one also speaks of the intestinal brain, they also have the same system of tight junctions, albeit with significant differences that are of great importance for detoxification of the CNS: The intestinal tissue is epithelial tissue, so it is in direct contact with the “outside world”, whereas the BBB is endothelial cells, i.e. there is no direct contact with the “outside world” at all. The special morphological and biochemical properties of the cell tissue of the brain capillaries are also very different from those of the intestine. The tight junctions of the intestinal mucosa are far less dense than those of the brain capillaries. Because of its high density, the tissues of the BBB are also called continuous endothelium. I refer to this level of detoxification as the “detoxification of the innermost of the innermost”.
The endothelial cells of the brain capillaries are additionally surrounded by a dense tissue layer of pericytes, which share a common basement membrane with the endothelium. Their task is, among other things, to regulate blood pressure locally independently and to form a kind of “second line of defence”. It is capable of phagocytosis and of presenting antigens to keep neurotoxic substances away. The common basement membrane of the BBB contains two different membrane systems with different enzymes, electrical polarisation and functions: the abluminal membrane facing the brain and the luminal membrane facing the blood vessel. With its abluminal side, the basal lamina borders the plasma membrane of the end feet of astrocytes, which in turn seal off almost 99 % of the two underlying cell tissues, the endothelium and the pericytes. Astrocytes are star-shaped macroglial cells which, with their projections to the neurons, serve to nourish them. With the so-called astrocyte swelling, they are responsible, among other things, for headaches during detoxification reactions.
The tight junctions of the endothelial cells not only close the intercellular gap between the cells, but also constrict the cells on all sides with their belt-like enclosure, so that the mutual membrane diffusion is also impeded. As a result, each of these layers is potentially capable of preventing the transport of solutes in both directions. Molecules wishing to pass through the BBB must pass through these two membrane layers, each with its own different properties. For example, supportive transport systems exist in the luminal membrane, while they are absent in the abluminal.
The membrane potential of the BBB has a comparatively high electrical resistance of 1,500-2,000 ohms per cm2. Adipose tissue is 500-1,000 ohms. Only the kidneys have a greater resistance (>6000 ohms). In comparison, the resistance of the mesenteric capillaries is only 1-2 ohms per cm2. The number of mitochondria in the endothelial cells of the brain is also particularly high. It is five to ten times higher than in other tissues.
The high number of mitochondria, the high blood flow and the high electrical resistance of the membrane systems illustrate why our brain reacts so sensitively to a lack of oxygen and energy and to toxic substances. Both active and passive transport depend essentially on the electrolyte balance, pH milieu, enzymatic conditions and oxygen partial pressure. The electro-chemical reduction of the membrane potential, for example through electrolyte imbalances, has similarly fatal effects on the barrier function of the tight junctions in the BBB as on those of the intestinal mucosa, but is far more electrolyte-sensitive in the brain than in the intestine.
The exchange of substances in both organ systems is impeded in both directions or facilitated for neurotoxic substances in the direction of the cell and cell subsystems when the voltage drops.
A circumstance that should give pause for thought, for example, in the case of EDTA chelation therapy, which results in a downright thinning of the electrolyte balance. The belief that a nutrient solution along the lines of that used by Dutch tomato farmers would remedy this situation is naïve in my view. Active transport at the BBB, which was considered impossible only a few years ago, can only be maintained with a very high enzymatic and energetic effort that stabilises the pH milieu and electrolytes. Therefore, I recommend that detoxification should always be accompanied by active cell-stimulating and cell-regulating measures with the help of microcurrents (MET) or similar systems.
The multi-stage regulated safety system of the BBB applies especially to water-soluble substances (hydrophilic), while it allows fat-soluble (lipophilic) substances to pass through relatively easily. Such a barrier system has advantages with regard to fat-soluble vitamins or other lipophilic substances, whereas hydrophilic substances such as glucose or water-soluble vitamin C or those of the B-complex are only allowed to enter through special transport systems. Unfortunately, this higher diffusivity also applies to all fat-soluble poisons such as nicotine, heroin or organic mercury.
1.3.2. The three phases of biotransformation
Roughly speaking, the disposal of toxic substances in mammalian biological systems occurs in a three-stage process sequence called the process of biotransformation. These are:
- Phase I reaction: activation and functionalisation of the compound.
- Phase II reaction: Conjugation of the compound activated in phase I with mostly hydrophilic, charged molecules.
- Phase III reaction: Binding of the hydrophilic substrates to transporters and transfer for excretion via kidneys, intestine or skin.
In the textbooks, only the concept of biotransformation phase I + II can be found. Since the introduction of the phase III reaction by Dr. Klinghardt, however, it is no longer possible to imagine naturopathy without it. Phase III in particular is responsible for many initial reactions when the excretory systems are overloaded. We experience these processes in daily practice as so-called Herxheimer reactions.
The primary task of the phase I reaction (functionalisation) is the chemical modification of the substrate by oxidation, reduction or incorporation of a functional group, e.g. by hydrolysis, with the aim of increasing the substrate’s solubility in water, deactivating potentially harmful biological activities and at the same time preparing it for the phase II reaction (conjugation).
The enzyme groups that are catalytically active in phase I are called oxygenases and are further subdivided into the groups of di- and monooxygenases (MO). For example, tryptophan-2,3-di-oxygenase plays an important role in metabolic disorders of the brain. The best known of the MOs is the large group of cytochrome P450 isozymes, of which there are more than a hundred different types with various subfamilies. They are localised in the endoplasmic reticulum and are found in high concentrations in the perivenous hepatocytes of the liver lobules, in the blood-brain barrier, but also, for example, in the renal cortex, where they serve the biosynthesis of steroid hormones. The enzymes of the cytochrome P450 families are less substrate-specific and are responsible for a large part of the detoxification reactions in the conversion of lipophilic to hydrophilic substances.
However, some catalysis processes involving MO produce toxic intermediates that are far more dangerous than the parent product itself, which can massively undermine detoxification. Some of the enzymes involved in biotransformation, e.g. glutathione S-transferases, also have a brain-specific isoform. Due to the chemical modification to increase their hydrophilic character, toxins can more easily overcome the BBB with the help of such enzymes and must be bound and neutralised before they reach the brain. It should additionally be noted that the brain, due to its high metabolic activity, also has an increased glutathione activity to reduce oxygen radicals.
The common word of the famous “shunting yard” in many detoxification actions and the massive danger of an increased toxic load on the brain becomes biochemically tangible here.
In order to understand the formation of these highly toxic metabolites from the functionalisation of phase I, one must distinguish oxidation as a catalytic reaction of MO such as cytochrome P450 from an oxidase reaction, as this is used here in deviation from its general meaning: While normally no oxygen atom is transferred, it is just the other way round in the oxidation of oxygenases. They ensure that oxygen atoms or, as in the case of MO, an oxygen atom is also incorporated / becomes incorporated into the substrate molecule, while the other is reduced by hydrogen. This results in an intermediate product that contains highly reactive atomic oxygen and is itself increasingly capable of oxidising other substances. In order to buffer such reactions and protect the organism from the cell-toxic effect of such metabolites, important co-factors are needed in detoxification such as antioxidants, trace elements and minerals.
Detoxification should not be initiated without sufficient antioxidant capacity (AOK), acid-base regulation and the targeted opening of the excretory pathways (this includes, in addition to intestinal cleansing, above all the pH milieu control of the kidneys).
After preparation through activation and functionalisation in phase I, conjugation of the substrate occurs through its linkage with a polar substance in the phase II reaction. Such coupling can take place as glucuronidation (glucuronic acid), as sulphation (sulphuric acid), as acetylation (acetic acid) or via amino acids such as taurine, glycine or peptides such as glutathione. The aim of phase II is to increase the hydrophilicity and further reduce the toxicity and thus prepare for the final step, the phase III reaction, in which the actual elimination of the water-soluble substance is to take place through specific transporters or carrier systems.
Ideally, the noxious substances are transferred via ATP-dependent efflux pumps into the bloodstream, where they can then be excreted via the lungs, kidneys, intestines and skin. However, other dangers lurk along this path. The most dangerous among them, apart from the already brain-specific problem, is the danger of heavy metals and other noxious substances precipitating into the kidney tissue. They must therefore be fixed with the help of special, firmly binding expelling agents. The task of such noxin carrier systems is to bind the end substrates more firmly than is normally the case via phase II conjugation.
The only person who has so far drawn attention to this and integrated it into his excretory procedures from the very beginning with the help of chlorella algae was Dr. Klinhardt (phase III reaction described above). The less dangerous, but still worrying danger is that of reabsorption via the intestinal mucosa due to its deconjugation by bacterial activities in the intestine as well as the lung detoxification functionally related to the intestine. To prevent reabsorption via the portal vein and precipitation of the end products from phase II in the kidneys, suitable binding agents must be administered for the orderly course of the phase III reaction (elimination).
The cascade of enzymatic reactions of the biotransformation of toxins in the mammalian organism has far-reaching consequences.
The rough division into three parts should not obscure the fact that many intermediate steps, for example in the cytochrome P450 reactions, have not yet been fully researched and that deficiency states with effects on the electrolytes, the pH milieu and the individual nutrient situation are added. Accordingly, we encounter a series of detoxification reactions or mobilisation crises, some of them most violent, distributed over the various barrier systems, excretion levels and compartments, which are not dissimilar to basic intoxication but increase in virulence when detoxification measures are initiated.
I would like to systematise these reactions somewhat below:
- Headache (TCM: “ascending liver fire”, orthodox medicine: astrocyte swelling with overload of ammonia detoxification in the brain).
- Serum: chills, fever due to increased virulence of plasma toxin load
- Vessels: burning veins, vasculitis
- Skeletal muscles: cramps due to electrolyte deficiency and toxin load, muscle pain
- Kidneys: Kidney pain, burning on urination, urethritis.
- Gastrointestinal tract: abdominal cramps, diarrhoea (shortening of intestinal transit as a natural counter-reaction), constipation, colitis
- Rectum: haemorrhoids, fissures, proctitis
- Lungs: coughing, asthma attacks, respiratory infections (often intestinal detoxification is not sufficient and leads to stress on the lungs)
- Skin: acne, itching, redness and swelling (bile acids), boils – here, too, the intestinal detoxification capacity is decisive.
In these cases, the binding capacity is too low and the AOK is insufficient, i.e. pH environment stabilising, intestinal cleansing, kidney supporting as well as liver protective measures must be extended.
2. Common methods of elimination
When characterising different agents and procedures, one must first distinguish between (1) solution, (2) opening of transport pathways, (3) active transport and (4) binding properties towards noxae. A final and very important question finally revolves around the reaction space in which the respective agent can be active. Is it serum- and / or cell wall-active or “only” intestine-active? Does it overcome the BLS / BHS and is it also suitable for bone elimination? Of course, the abundance of these questions cannot be fully answered in an overview, but can only be summarised in key points. Details may follow elsewhere.
2.1. The classic: wild garlic-coriander tincture and chlorella algae
I have worked successfully with this nutrient-based method for many years before I got to know simpler and more effective methods. Nevertheless, the Klinghardt method has not lost its charm. The purpose of this multi-stage procedure is first of all the opening of the ion-bound membrane systems for facilitated diffusion as well as the coupling of thiol groups with the noxae through a wild garlic-coriander tincture. Experience has shown that coriander, a herb used primarily in Thai cuisine and in Mexico, is an effective therapeutic agent for initiating the elimination of mercury and aluminium, also and especially in the CNS, even if this cannot be “proven” according to the usual criteria of orthodox medicine. However, coriander, whose effect is obviously based on bioflavonoids, merely opens the ion channels of the membranes for facilitated diffusion without transporting or binding noxious substances itself. The charge gradient of the membrane systems between the compartments of the EZR and the IZR is therefore decisive for passive transport. The former must have a lower toxicity than the IZR to enable transport across the charge gradient of the respective matrix.
The lower the degree of saturation and thus charge in the EZR, the easier the ejection. Purification of the Pischinger space should therefore be carried out upstream or in parallel.
Wild garlic, like many other bioavailable sulphur groups (MSM or raw leek vegetables), provides thiol groups that are able to bind heavy metals to themselves. In addition to these two tinctures, the binding agent is needed to eliminate the noxious substances via the intestines. The freshwater algae Chlorella pyrenoidea is used for this purpose. Compared to Chorella vulgaris, Chlorella pyrenoidea has a higher content of the active substance sporopollenin, which is responsible for binding.
The benefits of chlorella are numerous: binding not only heavy metals but also other noxious substances. It contains the bioavailable form of vitamin B12, methylcobalamin, as well as numerous minerals and trace elements, and also stimulates the TH1 pathway in the immune defence. However, several problems can also arise with this procedure:
- If the toxin load in the EZR is too high, the facilitated diffusion cannot unfold its effectiveness despite the opening of the ion channels by coriander due to the lack of charge gradient – on the contrary, it can lead to a massive influx of toxins into the cell if the ion channels are open – with fatal consequences for the patient.
- If the discharge quantity is higher than the binding capacity of the algae (difficult dosing), there is a risk of intestinal reabsorption.
- Chlorella algae are “only” active in the intestine, i.e. they are neither serum- nor cell wall-active, so that in addition to the danger of intestinal reabsorption, there is also the danger of free noxae in the serum, which are then fed to the kidneys, where they can certainly damage the kidney tissue.
- Plants with an affinity for heavy metals naturally have a high affinity for toxins, so that the purity of the algae is important in order to avoid, for example, the high arsenic content often tested in chlorella algae.
Further limitations of this method are that it is not possible to eliminate higher-value synthetic noxious substances such as polychlorinated biphenyls or radioactivity. Bone elimination is also not possible. The intake routines are somewhat complicated, at least for older people (change of tincture, pauses for excretion and chlorella dosage). With higher doses of algae, allergic reactions can also occur due to the high protein content (leaky gut). Chlorella is contraindicated because of its iodine content in thyroid diseases and disorders of iron utilisation and too low transferrin because of its iron-binding properties. Another, not insignificant factor is the fact that plants with an affinity for harmful substances do not limit their ability to bind noxious substances to mammalian organisms, but also bind them in the wild. This often leads to the fact that the detoxifying substances are already heavily saturated with heavy metals and other noxious substances. It is imperative that the plants used are purified before administration or that the initial contamination of the plants is checked.
2.2. Half measures: Bioresonance Therapy
Military men all over the world have always known it: marching music increases the pulse rate and thus the blood circulation, which in turn naturally contributes to detoxification. As with increased exercise, it acts as an important activator of blood and lymph flow and, when combined with sweating, leads to increased elimination of harmful substances. The basic cell-stimulating effect – but without sweating – is also the basis of bioresonance therapy. However, due to the biochemical reaction steps described above, it is strongly advised not to use this method alone with people who are heavily poisoned. Especially when it is not certain whether anitoxidative capacity (AOK) or even the detoxification capacity itself is guaranteed. The belief in the single and omnipotent spirit of vibrations can very quickly lead to disillusionment due to the effectiveness of the factual. This also applies to the numerous diets on the market, which do not take into account that they dissolve toxins from the tissues as a catabolic process and then hope that the Lord God will take care of it, if the therapist even thinks about it. However, if the dissolved toxins are not specifically bound with substances with an affinity for harmful substances and excreted, or if the patient is a poor excretor or detoxifier (polymorphisms phase I + II), there is a danger of transfer to other fatty tissues, in the worst case to the brain (shifting station).
As a supporting measure, bioresonance methods, similar to acupuncture and other cell-activating methods (homeopathy), are, however, excellent instruments to accompany detoxification. Protracted detoxification processes can be considerably shortened in this non-invasive way.
2.3. The dangerous ones: EDTA, DMPS, DMSA.
All chelating agents (from the Greek word chelus for “claw”) bind metal ions, which is the purpose of the exercise. Therefore, different parameters are crucial for their evaluation and use. First of all, this applies regardless of whether they are more hydrophilic or lipophilic and thus blood-brain barrier (BBB). The most important criterion for the binding properties, apart from the binding strength, is the order of binding, since minerals and trace elements are also metallic, but these are necessary for maintaining a stable membrane potential, especially at the sensitive BBB. The decisive question is therefore whether chelates tend to bind in ascending order within the periodic table, as is the case for the chelates of EDTA, DMPA or DMPS, or whether they bind in descending order of molecular weight, as in the case of low-molecular-weight pectins (micropectins such as PektiClean®), which bind heavy metals and molecularly higher-weight noxious substances first. In the first case, valuable minerals and trace elements are bound and eliminated long before the first toxin is bound, which usually results in a massive impairment and disturbance of the electrolyte balance. With quite threatening toxic effects accompanied by side effects during the detoxification process. The generally persistent criticism of these forms of excretion is therefore more than justified and should not only be heard through the fears of patients who have had bad experiences with them. It is not opportune to simply brush such concerns aside with reference to therapist competence.
Another aspect of chelates is their binding strength, i.e. the possibility of chelates dissolving in the renal tissue under certain physiological conditions such as acidic pH environment, glucose and protein content, osmolarity, glomerular filtration pressure, etc., and leading to the precipitation of toxins in the renal parenchyma, for example. Possible long-term damage is often not immediately detected by the usual blood analyses.
EDTA (ethylene diamine tetraacetic acid anion)
EDTA are salts of ethylene-diamine-tetraacetic acid. In addition to the two free electron pairs of a nitrogen atom, they can provide four carboxyl groups for a complex compound, i.e. bind sixfold to a cation. In this way, it is able to form relatively stable complexes even with those cations that have an extremely low tendency to form complexes, such as calcium. The free acid is poorly soluble, especially at low pH, whereas the salts are very soluble in water, but not in fat. This makes this method unsuitable for CNS detoxification, as EDTA cannot pass through the BBB. The fact that EDTA first eliminates valuable mineral salts is one of its central problems. In addition to calcium, EDTA binds particularly stable complexes with Cu, Ni, Fe, Co and Zn. This cannot be compensated for even by the administration of simple nutrient solutions and leads to an electro-chemical depletion, which, among other things, also explains the numerous side effects and contraindications. Especially for the high electrical resistance of the membrane systems of the BBB, this means an inferno.
The EDTA procedure was developed in the 1960s in the course of acute lead poisoning as an emergency measure – and (only) there it belongs in my opinion. Many naturopathic therapists complain again and again about the transfer of accident and emergency medicine therapy procedures by orthodox medicine to chronic processes – and here we are doing exactly the same.
In an emergency, some risks may be acceptable, but this is not the case in the treatment of chronic diseases, especially since there are more efficient, less dangerous and, what is more, non-invasive procedures. Incidents involving fatalities are allegedly only recorded in the early years and during the period of dosage discovery. Let’s take a closer look at this supposedly “non-toxic and low-risk” infusion in terms of recorded incidents, its recognised side effects and its contraindications:
- Adverse events: Hypocalcaemia with tetany, allergic reactions up to anaphylactic shock, renal failure, cardiac arrhythmias, bone marrow depression, necrotising injection wound.
- Side effects (see my scheme of mobilisation crises in case of inadequate purging procedures): Chills, even six to eight hours after infusion, to temperature rise and chills, minor heart pain, burning pain at the infusion site and carried on in the arm, burning of the veins, dizziness, aching limbs, backache, thirst, weight loss, fatigue, herpes, migraine, head pressure.
- Contraindications: Kidney and liver dysfunction (not only severe), heart failure, cardiac arrhythmias.
In addition to the negative balance with regard to the primary binding of valuable alkali and alkaline earth metals, which also applies in a limited form to DMSA and DMPS, there is also the relatively low binding power of these complexing agents. So before chelates bind mercury, the person is not only electrolytically “empty”, he is also exposed to the danger of toxins precipitating in the renal parenchyma. The administration of NaMg-EDTA as a mineral substitution, i.e. an electrolyte solution, is not sufficient in my view. Without full stores of physiological cations, EDTA infusion is contraindicated from the outset. The substitution must take place beforehand and be monitored in the laboratory.
In addition, there is a complex monitoring of the kidneys, in which, in my opinion, even cystatin C is not sufficient for the glomerular filtration rate, as bio-resoance analysis procedures and frequent diagnoses of silent inflammations show. Cystatin C is certainly more sensitive as a renal marker than the creatinine value, but also shows itself to be elevated in rheumatism and hypothyroidism.
Since EDTA is a pronounced calcium eater, cardiac arrest can even occur without prior substitution (cardioplegia). In addition, the more acidic the environment, the lower the binding affinity of EDTA, i.e. it robs valuable bases, but only binds under alkaline conditions – a vicious circle. Detoxification from clearly acidic compartments (pH <6.5) is hardly possible with the chelators mentioned. But how is this supposed to work with the usually acidic metabolic situation of poisoned patients? If the (post-) glomerulolar pH is below 6.5, there is a risk of premature release of the bound toxic cations into the renal parenchyma due to the poor binding power of EDTA, DMPS and DMSA. And which toxically burdened person does not suffer from acidic, often also renal acidic disorders at the same time? In addition, the so-called renal blockage only sets in from pH 4-4.5. In order to circumvent such an acidic situation ex ante, the kidney increases glutaminase in order to alkalinise the tissue via additional ammonium ions. This can lead to a secondary acidosis in the case of renally induced alkalosis of loss. To compensate, however, the kidneys temporarily reduce urea excretion, similar to the starvation metabolism, so that this leads to a congestion in the ammonia detoxification of the liver, which, for its part overloaded, releases the whole thing into the bloodstream (feeling cold, fever) and is passed on to the brain as “rising liver fire” (TCM). The liver and kidneys work closely together in the ammonia detoxification via the urea cycle. Our brain, which has comparatively little capacity for ammonia detoxification, is the first organ to suffer from even slightly elevated ammonia levels.
The whole thing stands and falls with the pH-dependent collloid-osmotic pressure in the renal parenchyma. And what chronically ill patient has perfectly healthy liver and kidney values?
This means lots of contraindications: Glomerulonephritis; diabetics, in whom the glucose load is too high, which also increases the colloid-osmotic pressure and thus the risk of nephrotoxic reabsorption; proteinuria: here, too, the colloid-osmotic pressure increases due to the proteins and thus the risk of reintoxication of the renal parenchyma because of the very loose chelate binding.
A correspondingly unfavourable charge gradient due to pH milieu can lead to the accumulation of heavy metals in the tubule cells and thus to intracellular heavy metal poisoning, which may not be noticed until years later. Electrolyte deficiency, anaemia, liver and kidney diseases are also clear contraindications to EDTA detoxification. I personally know only a few therapists who make the kind of effort in follow-up that is required for these procedures.
DMPS (dimercapto-propane sulfonic acid)
DMPS is a sulphuric acid salt with free SH groups that bind certain heavy metals, but also “positive” metals in the periodic table in ascending order (= copper, zinc and iron BEFORE mercury), i.e. a strong demineralisation and trace element depletion takes place. Like EDTA, it is usually given intravenously, requires a prescription and can also be taken orally if its effect is reduced. Its absorption rate is 50% orally, according to studies. It is not suitable for cerebral detoxification because it is hydrophilic and cannot pass through the BBB. It also only acts extracellularly, so it cannot reach metals in the cells. In addition, as with EDTA, bone detoxification is not possible. DMPS orally also contains titanium oxide (E171), which is very questionable as it is said to have a carcinogenic effect (Cf. Mutter, 2009). Mutter, a convinced supporter of DMPS, recommends DMPS ampoules also for oral use, otherwise subcutaneous administration. However, there is a risk of increased toxicity for the liver and kidneys, i.e. if at all, detoxification is only therapeutically justifiable with healthy kidneys. The same applies, of course, to the risks of an acid renal situation, increased glucose levels in the urine and proteinuria. Allergic reactions as with EDTA, but in a weakened form, are known.
Side effects (according to Rupprecht, 2008):
- Hypotensive effects if administered i.v. too quickly.
- High allergy potential
- Interactions especially with essential trace elements such as Cu and Zn.
DMSA (dimercapto succinic acid)
For a long time, DMSA – in contrast to the other two chelates – was considered lipophilic, which should have been an advantage in cases of poisoning in the cerebral area. However, like DMPS, it is water-soluble and has no cerebral detoxifying effect. In addition, it has a lower absorption rate when given orally than DMPS (20%) and according to a study by the laboratory of Dr. Bayer (2008), DMSA administrations are associated with a higher risk of side effects (Dr. Bayer, 2008) Its sulphur ends primarily bind Hg, less so other heavy metals. The metal affinity is more positive than with DMPS: Cd-Pb-Fe-Hg-Zn-Ni, i.e. mercury binding is already quite rapid, with major problems in the area of iron. Otherwise, the same applies to its binding strength and the danger of precipitation into the renal parenchyma as to its two colleagues. The “chelate industry” has known about these problems for many years, but does not communicate them because economic interests are in the foreground.
Side effects (cited, after Bayer, 2008):
- Gastrointestinal symptoms in up to 20% of patients: Vomiting, diarrhoea
- General symptoms such as headache, backache etc. approx. 15%.
- GOT and GPT elevations in approx. 10% of patients
- Moderate neutropenia in approx. 1-2%.
- Arrhythmias, approx. 2%
- Paraesthesias
As a summary one can state: DMPS seems to be less afflicted with side effects and is preferable to the administration of DMSA, provided that the problem of acidic renal conditions and the associated danger of precipitation of the chelated metals is taken into account, as well as of course the trace element and electrolyte depletion, which should not be neglected, especially in chronically ill patients. Dr. Mutter recommends in any case an additional mineral and selenium supplementation of up to 3,000 µg selenium in the form of an HG-selenide complex.
There is a big difference between first impairing a patient’s electrolyte balance, which is elementary for self-regulation, through excretion methods and then restoring it, or vice versa through a suitable combination of intestinal cleansing, acid-base regulation, increasing antioxidant capacity, liver-protective measures by reducing the amino-nitrogen load, etc. Detoxification measures prepared.
2.4. The gut actives: Zeolites and chitin
Zeolites
Zeolites are highly functional bioregulators – especially clinoptilolite zeolite. They consist of the basic building block SiO tetrahedron, i.e. a central silicon atom and four oxygen atoms. Thus, it contains the two most abundant elements in terms of quantity, oxygen and silicon. Zeolites are neither serum- nor cell-permeable, but are intended exclusively for intestinal detoxification. Besides silicate, they also contain aluminium (Al), which, however, is not bioavailable but firmly bound, so that it can only dissolve in the organism under extreme conditions. A very high thermal effect is required to dissolve this stable compound. Frequently raised objections against zeolites with regard to aluminium are therefore unfounded. However, the use of zeolites is still not advisable in cases of leaky gut syndrome, as GALT-mediated (Gut Associated Lymphatic Tissue) can cause an antigen-antibody reaction against aluminium, even if it is bound.
Zeolites are definitely a useful supplement for the detoxification of heavy metals in the intestine as long as there is no leaky gut.
However, due to their exclusive intestinal activity and their extensive restriction to heavy metals, zeolites alone are not sufficient for a meaningful detoxification in all three barrier systems.
Chitin
A relatively little known but nevertheless very interesting substance is the colourless, tough biopolymer chitin (Greek chito = “undercoat”, “shell”, “carapace”), a natural oligo-glycoprotein found in the chitin shell of shellfish, which is derived from chitin. It can also be obtained from some fungi of the order Mucoraceae (e.g. Mucor rouxii, Absidia coerulea or Rhizopus oryzae).
Chitin, like cliniptilolite, is neither serum- nor cell wall-bound, but is “only” active in the intestine. The solubility in acids and at the same time poor solubility in neutra-leic or alkaline pH is unique among biopolymers and therefore characteristic. It is therefore active under renal acidic conditions as well as and especially in the intestine under acidic conditions. With decreasing molar mass, chitin is also soluble in water and even in alkalis. Due to its free amino groups, it behaves as a poly-cation with a high charge density in non-alkaline solution.
The great advantage of chitin is its lipophilicity, which is why it is especially able to bind noxious substances bound to fats in the intestine. It is non-toxic, antibacterial, antiviral and anti-allergenic, which also makes it good for use in the intestines of leaky gut patients with a high antigen-antibody reaction. Furthermore, it has haemostatic and fungicidal effects. Besides lipophilic toxins, it can also bind inorganic heavy metals.
2.5. The all-rounder: low-molecular pectin
Low molecular pectins (nP) or micro pectins are a relatively young class of chelates of biological origin. Pectins are found in many plants, fruits or vegetables and are an integral part of our diet. They have a positive influence on blood sugar and cholesterol levels and are effective against toxic stress. In nature, however, pectins only occur in combination with other substances, which is why they are then called high-molecular or macropectins. Therefore, for therapeutic application, low-molecular pectins must be strictly distinguished from their “high-molecular brothers” from apple, pineapple or citrus fruits, which are only intestinally active but not serum and cell wall active like the low-molecular forms. High-molecular-weight pectins thus have a limited (restricted to the intestine as a compartment) and lower efficacy. Another important distinguishing feature within the low-molecular-weight pectins is their highly variable proportion of low-molecular-weight mass, ranging from 8 to 60 % (as in PektiClean®).
Low molecular weight pectins act as highly active polyanionic adsorbents and can bind and eliminate heavy metal ions, bile acids and pathogenic microorganisms (including its direct inhibitors) as they pass through the gastrointestinal tract. They also exhibit significant levels of antidotal, cholesterol-lowering, antibacterial, hepatoprotective, anti-inflammatory and anti-allergenic activities. Upon entering the bloodstream and other organ tissues, low molecular weight portions of pectin come into direct contact with the receptor structures of cells (some immunocompetent), which in turn induce reactive changes in the status of the cells. Blood tests in Russian studies regarding the effect of nP on the cells revealed, among other things:
- Stimulation of T and B cells,
- Increase in the number of antibody-producing cells,
- Intensification of the delayed type of hypersensitivity,
- Induction of spontaneous proliferation of splenocytes.
Low molecular weight pectins also appear to exert an inhibitory effect on the induction and formation of T suppressors and appear to be able to increase the functional activity of suppressor cells. The low-molecular components of pectin can bind various harmful substances directly in the bloodstream and subsequently be excreted with them via organs such as the liver and kidneys.
Pectins themselves are polysaccharides that consist of α-D-galacturonic acid with up to 65 % of their mass. The anionic charges along the macromolecules resulting from this compound are the cause of their high binding capacity for cations. The polymeric chains thereby form a sequence of negative charges that bind positively charged exo- and endotoxins. They are also able to bind higher-value synthetic noxious substances and radioactive substances.
Comparison between high and low molecular weight pectins

Fig. 1: High-molecular pectins like apple or pineapple pectin (dark green particles) are not able to diffuse the cell wall. They therefore act “only” in the intestine. Due to their size, the surface area is relatively small, thus their binding power is also lower.
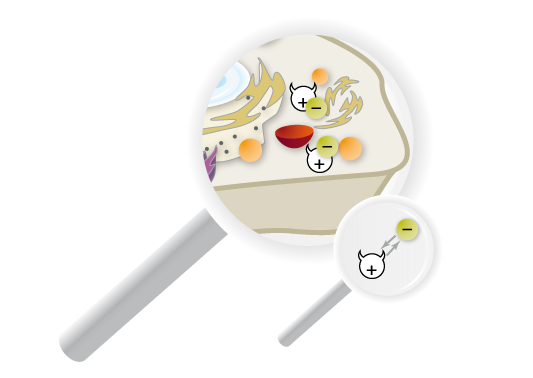
Fig. 2: Low-molecular pectins (light green particles) create an extremely strong bond to a polar substance. They are also and especially effective under acidic renal conditions and “without damaging renal tissue” (Burgerstein). Due to their small size, they can penetrate the cell wall and have a relatively large surface area, so that the binding power is also many times higher in terms of quantity.
What has been said about low-molecular pectins brings some essential differences to the chemical chelates mentioned so far:
- Low-molecular pectins are also and especially effective under acidic renal conditions. They even develop their optimum effect here. Moreover, they are tiny and have a correspondingly large surface area, so that their binding capacity is many times higher than that of high-molecular chelates. Their use is therefore particularly recommended for diseases of the urogenital tract.
- In contrast to many other chelates, they form an extremely strong bond which does not dissolve in the kidney even under the pathological conditions mentioned. Due to their low molecular weight, they can easily pass through the renal tubules. Since the majority is eliminated via the kidneys – with a simultaneous alkalising effect in the renal parenchyma – nP can be used preferentially, especially in the case of problems of the intestinal tract (leaky gut). And from my experience, they can be used efficiently for detoxification of the CNS, despite their water solubility, together with mobilisation via microcurrent.
- Since the binding takes place in descending order in the periodic table, it also spares valuable alkali and alkaline earth metals as well as trace elements, so that calcium substitution only has to be recommended for longer intake (>1 month). In addition to detoxifying the CNS, nP are also suitable for radioactivity and for bone elimination. nP also have hepatoprotective properties due to their ability to break enterohepatic cycles by supporting the cascade of biotransformation I to III already at levels I and II. Only under highly alkaline conditions is the effect of low-molecular pectins limited, which is why an additional dietary fibre component is recommended for intestinal detoxification, especially in cases of intestinal overbasing, for example as a result of increased proteolysis (putrefactive flora) by protein-decomposing bacteria or by increased urease of certain bacteria capable of urea cleavage and ammonia recovery.
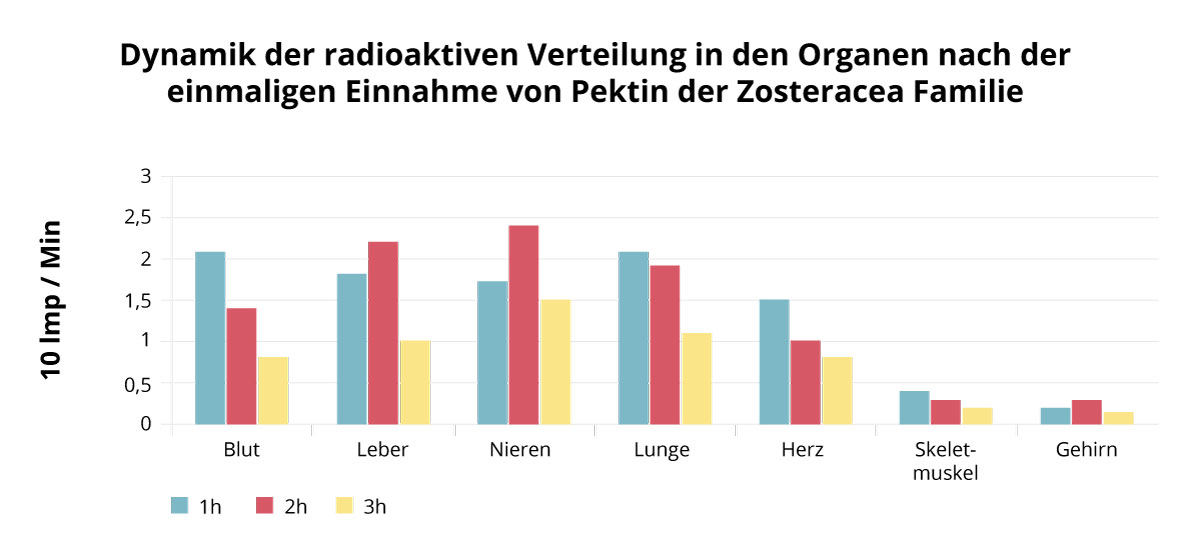
Analysis of the radioactive distribution of nP revealed the following results:
Special contrast media make it possible to trace the dynamics of radioactive elimination in organs and tissues. One hour after the administration of the contrast medium and the ingestion of low-molecular pectin, it becomes visible that the radioactivity has concentrated mainly in the blood and lungs, after 2 hours in the liver and kidneys. The increased absorption of the radioactive material in the liver and kidneys is followed by a strong decrease in radioactivity. This is undoubtedly related to the excretory function of these organs. In the brain and the skeletal muscles, a comparatively low specific activity could be shown, which may also be related to the lower exposure.
3. My royal road: the combination of Human Amino Acid Profile (MyAMINO®) and PektiCLEAN® with microcurrent therapy (MET)
Up to now, methods of excretion have been described, all of which were rather passive in character as far as the cell activation itself is concerned – with the exception of bioresonance therapy. However, the electro-chemical membrane potential is not only determined by the electrolytes and the pH milieu, but also by movement as well as by the guiding signals of the environment: magnetic field, sun, Schumann frequency, etc. These contribute to the body’s electrostimulation. They contribute to maintaining body electricity and mass transfer. As we have seen, the resistance of 2,000 ohms per cm2 in the membrane systems of the BBB is extremely high, so that in practice it has proven to be extremely beneficial to support this “body electricity”, as Dr. Robert O. Becker, one of the founders of microcurrent therapy, calls it, with the body’s own healing currents. I myself have developed a combination of several interlocking building blocks within the framework of my metabolic pogram of dr. reinwald metabolic regulation, all of which aim to improve detoxification measures. The most important of these are the following basic elements:
- Micro-current or micro-energy therapy (MET) for the regeneration of cellular energy.
- Use of the unique amino acid pattern Human Amino Acid Profile (MyAMINO®) to relieve the detoxifying organs (provides almost no nitrogen waste and no glucose)
- Low-molecular pectins such as PektiCLEAN®
- Intestinal cleansing (floral strengthening with pro- and prebiotics) and intestinal detoxification with chitin products (e.g. ChitosaCLEAN® colon or ChitosaCLEAN® fungus
- Improvement of the AOK (e.g. with minus-charged hydrogen as in Active H®) as well as build-up of mineral and trace element depots (e.g. in VitalBASE®)
- Isomedical therapy according to Enderlein/Haefeli
With the help of micro currents during micro energy therapy (see my essay: MET – Basis of a Regulation of Cell and Milieu) we induce body-analogue healing currents (control and injury current) together with organ-specific frequencies. In this way, we open up and support the organs that are discharging.
MET aims at the activation of cell and environment and thus also at the improvement of the function of organelles such as the mitochondria, which are actually symbiotic bacteria (see my essay: Mitochondriopathy: A new explanatory model from the prison of thought of cellular pathology or a possible bridge to humoral pathology?)
With MET applications, we improve the exchange of substances between the cells by, among other things, improving the membrane voltage (capacitive resistance in ohms). According to in vitro studies, microcurrent provides an increase in ATP production of up to 500 % and also an increase in protein synthesis of up to 73 % and membrane transport of up to 40 %. At the same time, anti-inflammatory processes are initiated by such MET application, as Dr McMakin was able to show in studies. If such systems are combined with serum- and cell wall-active as well as intestine-active substances that reach different types of noxious substances in different barrier systems (low-molecular pectins, zeolites and chitin are suitable here according to the above explanations), then, in all experience, very little stands in the way of successful support of the detoxifying systems, even in the difficult area of the CNS.
3.1. Protein metabolism, acid-base balance and detoxification
ammonia (NH3). Ammonium is the corresponding acid of ammonia. The acid strength of ammonium is very weak (pKS 9.25), so that under physiological pH conditions there is a large excess of the ionised form in the equilibrium of NH3 + H+= NH4+ in the plasma. Specifically, this means in the ratio of > 99% ammonium and < 1% ammonia. Ammonia can easily diffuse through cell membranes with the help of aquaporin (protein-bound water channels). Plasma concentration should be below 35 μmol/l. Many laboratories erroneously report higher values. However, ammonia has a neurotoxic effect at higher concentrations. Hyperammonaemia can lead to glutamine accumulation in astrocytes and cerebral oedema.
Our organism knows two main detoxification pathways to accomplish the detoxification of ammonia: urea biosynthesis and glutamine synthesis. Both metabolic pathways are embedded in the highly developed, structural and functional organisation of the liver acinar and, together with the kidneys and the lungs (as well as the connective tissue), are essentially responsible for the regulation of the acid-base balance. It is important to note the hepatic zonation, i.e. the different localisation of the two main pathways of ammonia detoxification.
Glutaminase takes place in the periportal hepatocytes and assumes an important pacemaker function for the urea cycle because it generates its own stimulation through the release of NH3 that it triggers. What cannot be converted into urea biosynthesis in zones 1 and 2 of the hepatocinus – high capacity with low affinity – is transported to the scavenger cells in the perivenous hepatocytes – zone 3 of the hepatocinus – where, with high affinity but low capacity, renewed NH3 fixation takes place via glutamnin synthesis, i.e. a kind of glutamine recycling. It is restricted to this subpopulation of hepatocytes, the scavenger cells, at the outermost edge of zone 3 of the hepatic acinar (distal), because they capture ammonia that could not be disposed of via the urea cycle (zone 1/2) in a kind of “final purification” and fix it again in glutamine. This is then transported to the kidney for further processing. There, amino nitrogen can be used to regulate the pH of the kidneys.
The serial arrangement of the two main detoxification pathways for ammonia in the three zones, in which the enzymatic processes are connected in series and in parallel at the same time, provides a complete and extremely safely designed detoxification system. This intercellular glutamine cycle in the liver and its involvement in SB homeostasis were only recognised biochemically and physiologically by conventional medicine in the 1980s. In the process, a small paradigm shift took place within mainstream medicine by moving from the two-organ model (lungs-kidneys) to the, in my view, still deficient three-organ model (lungs-kidneys-liver) in the acid-base process and placing the liver at the centre of the acid-base process. A development that is still not presented in most textbooks for medical studies. However, the role of the liver and the still unrecognised connective tissue in the acid-base process was already presented in detail by the clinician Prof. Dr. F. Sander in the 1930s and in his monograph in 1953. It took more than 50 years, with all goodwill towards this more recent development and its protagonists, until at least the role of the liver in SB homeostasis was officially understood. One can therefore confidently speak of the “discovery of the Mediterranean” within orthodox medicine with regard to SB events and the liver.
The detoxification of amino nitrogen by the liver is not only very energy-intensive, it consumes 3 ATP and an energy-rich phosphate compound per 1 mol of urea (NH2CONH2) produced. In addition, however, it also consumes 2 moles of bicarbonate (HCO-3). Thus, to remove the high alkaline load from amino acid metabolism, the liver consumes a large part of the buffer capacity in bicarbonate, which can react as both an acid and a base as a “both/and buffer” with an acid strength of 6.1 pKs. Urea biosynthesis disposes of the base ammonia (NH3) in the same proportion as it consumes hydrogen carbonate (HCO-3) (stoichiometry). With increasing alkaline load from amino nitrogen from protein metabolism, there is therefore also an increasing reduction in buffer capacity. The loss of bicarbonate cannot usually be completely compensated for by renal reabsorption, so that a loss acidosis develops. The resulting latent connective tissue acidosis with reduced buffer capacity was described very well by Sander in his book on the saline cycle, which is still worth reading. Behind the defence against dangerous alkalosis lurks the danger of metabolic acidosis. At the same time, the liver is able to react to metabolic alkalosis and metabolic acidosis in interaction with the kidneys. I.e. we have an interhepatic (hepatic acinar zone 1 to 3) on one side and an interorganic (liver-kidney) glutamine cycle on the other. In metabolic acidosis, the liver throttles the urea cycle, disposing of less ammonia but saving bicarbonate. In the opposite case of alkalosis, the urea cycle is cranked up and ammonia is disposed of with increased consumption of bicarbonate
Normal case:
Urea cycle = NH3 + HCO-3
Acidosis:
Urea cycle = NH3 + HCO-3
Alkalosis:
Urea cycle = NH3 + HCO-3
Due to the intercellular glutamine cycle, however, this process must be further differentiated into the areas of periportal and perivenous hepatocytes. In the case of acidosis, the lowering of the HZ in the area of the periportal hepatocytes leads to the saving of bicarbonate and increased ammonia, which is then fixed again in glutamine via glutamine synthesis in the area of the perivenous hepatocytes (Z 3) and transported to the kidneys, where it contributes to the release of ammonia and thus to alkalinisation or the reduction of acidosis in the kidneys. Conversely, the liver curbs glutamine synthesis under alkaline conditions and increases glutaminase activity (release of ammonia) in zones 1 and 2 of the hepatic acini. The pH is controlled by increasing or decreasing the extracellular pH. A decrease of the extracellular pH by 0.1 from the physiological value already inhibits the glutaminase-controlled ammonia production for urea synthesis by 70%.
3.2. Urea cycle and cytochrome P450 detoxification
Of particular importance for our considerations is now the inclusion of other detoxification measures. For in the perivenous hepatocytes not only glutamine synthesis takes place and the enzyme glutamine synthetase is localised, but also the lion’s share of the CytP450 family. If detoxification measures are initiated, either by the therapist or by the biorhythm of the organism itself, then there seems to be a reduced efficiency of urea biosynthesis, in that the liver increases detoxification via the CytP450 family and has to throttle the glutamine cycle between periportal and perivenous hepatocytes, since the liver works in a strictly hierarchical way. Obviously, the activity of biotransformation in the perivenous area increases at the expense of glutamine synthesis, which is why the latter cannot maintain its “cleaning-out” function to the full extent. In turn, the ammonia level increases (hyperammonaemia). At the same time, glutaminase in the periportal hepatocytes is increased in favour of the urea cycle to compensate for the lack of glutamine synthesis in the perivenous area, which in turn consumes more hydrogen carbonate. The result: the ammonia level rises. Since NH3 can diffuse more easily through the cell membrane, it penetrates more into the macroglial cells of the blood-brain barrier, even in the case of mild hyperammonaemia, and causes irritation there.
Fig. 3: Interhepatic and interorganic glutamine cycle. Glutaminase reaction in zones 1 and 2 of the hepatic acinar. Transfer of the lion’s share of amino nitrogen (NH3) to the urea cycle. Transport of urea to the kidneys for excretion. The escaped amino nitrogen (low affinity and high capacity of the periportal hepatocytes) is transferred interhepatically to the perivenous hepatocytes in the distal area of zone 3 of the hepatic lacinus (high affinity to amino nitrogen with low capacity), where the scavenger cells or “scavenger cells” convert NH3 back into glutamine via glutamine synthesis. With glutamine as a non-toxic transport amino acid, the bound nitrogen is transported to the kidneys, where the glutamine can again release its amino nitrogen via the glutaminase reaction to regulate (alkalise) the pH environment in the kidneys.
In such cases, TCM speaks of “ascending liver fire”, orthodox medicine of astrocyte swelling, and the patient of migraine or headache. Ammonia intoxication is part of the pathogenesis of hepatic encephalopathy. If, in addition, the Cori cycle is overloaded, in which the liver passes on part of the lactate supplied via the alanine cycle to the heart, which, within certain limits, is able to use lactate for its metabolism, then this also leads to lactic acidosis with a risk of oxygen deficiency (coronary vessels) or even infarction. TCM then calls this the “rising heart fire”.
The only ones who have reacted to this process so far, albeit in the wrong way, have been the fasting followers. They have reduced the protein load from food protein to relieve the liver and kidneys. But in doing so they have tried to cast out the devil with the Beelzebub. Because the radical reduction of dietary protein over a longer period of time – as in the Buchinger fast – leads to a lack of energy and glutamine and thus to a reduction in renal ammonium genesis, which the body now tries to compensate for from its own protein reserves: at the expense of lean mass (skeletal muscle, immune mass, organ cells). Protein catabolism during prolonged fasting leads to emaciation (starvation metabolism).
Protein deficiencies, however, are not conducive to detoxification. The supply of dietary proteins to maintain health is indispensable. And this is where the use of Human Amino Acid Profile (MyAMINO®) offers a great opportunity, as it enables us to relieve the detoxification organs and at the same time ensure a high protein supply. According to studies, MyAMINO® provides only 1% of nitrogen waste and 99% of net amino-utilisation value (NAV), in contrast to, for example, meat, fish and poultry with an average of 32% or vegetable proteins with a maximum of 18% NAV. On the other hand, this means between 68% and 82% nitrogen waste in animal and vegetable proteins.
Since MyAMINO® does not produce any digestive end products and can be completely absorbed in the small intestine without the need for proteases, it not only relieves the liver and kidneys, but also provides maximum relief for the gastrointestinal tract, while at the same time providing an optimal protein supply.
With MyAMINO® we are able to combine the partial benefits of fasting (reduced load of nitrogen waste from exogenous protein intake, reduced load on the digestive tract, reduced load on the cardiovascular system, physiological ketosis) with a healthy and vital protein supply by avoiding the dangers of prolonged fasting. In my opinion, this is what makes optimal detoxification possible in the first place.
Finally, I would like to remind you of a Chinese proverb that places the opening of the excretory tracts of the intestines and kidneys as a preparatory measure at the beginning:
“If you want to chase the tiger out of the house, open the windows and doors before you step on its tail.”
List of references
Bayer, Wolfgang: Durchführung, Referenzbereiche und Interpretationen des DMPS-Testes. Eine kritische Datenanalyse, Berlin, 2008
Becker, Robert O.: Körperelektrizität (The Body Electric), Leben Verlag AG, St.Gallen, 1999
Brenner, U. P.: Die Struktur der Blut-Hirn-Schranke und der Blut-Liquor-Schranke – eine Literaturstudie, Diss, Univ. München, 2006
Guder, W. G., Häussinger, D., Gerok, W.: Renal and Hepatic Nitrogen Metabolism in Systemic Acid Base Regulation, J. Clin. Chem. Clin. Biochem. Vol. 25, 1985, S. 457-466.
Häussinger, Dieter: Nitrogen metabolism in liver: structural and functional organization and physiological relevance, in: Biochem. J. (1990), 267, S. 281-290.
Häussinger, Dieter: Ammonia, urea production and pH regulation, in: Rodes Juan (Hg): The Textbook of Hepatology: From Basic Science to Clinical Practice, S. 181-192, 3rd Edition, 2007, Wiley-Blackwell
Horn, F.: Biochemie des Menschen. Lehrbuch für das Medizinstudium, 4. Aufl., Thieme 2009
Lucà-Moretti, Mauricio: A comparative double blind triple cross-over NNU study confirming discovery of the Master Amino Acid Pattern®, in: Annals of Royal National Academy of Medicine of Spain, Volume CXV, Madrid 1998.
Märten, S.: Proteomanalyse der Blut-Hirn-Schranke, Diss, Univ. Darmstadt, 2004
McMakin, Carolyn: Frequency Specific Microcurrent in Pain Management, Elsevier, Washington, 2011
Mutter, Joachim: Gesund statt chronisch krank! Der ganzheitliche Weg: Vorbeugung und Heilung sind möglich, Natura Viva Verlag 2009
Nelson, D. et al: Lehninger Biochemie, 4. Aufl., Springer 2011
Ruprecht, J. Dimaval. Wissenschaftliche Produktmonographie, Heyl, Berlin, S. 15-18
Sander, Friedrich F.: Der Säure-Basenhaushalt des menschlichen Organismus im Zusammenspiel mit dem Kochsalzkreislauf und Leberrhythmus, 1. Aufl. 1953, unveränd. Nachdruck 1985, 1999, Hippokrates Verlag
Schartl, M. et al: Biochemie und Molekularbiologie des Menschen, Urban & Fischer, 2009
Schilling, Florian: Praxisseminar I – Darmsanierung, 2010, unveröff. Arbeitspapier
Schilling, Florian: Praxisseminar II – Säure-Base-Haushalt, 2010, unveröff. Arbeitspapier
Schilling, Florian: Praxisseminar III – Entgiftung, 2010, unveröff. Arbeitspapier
Pankert, P.: Wirkung von Glucuronolacton – Proteomanalysen und Transportstudien an der Blut-Hirn-Schranke, Diss, Univ. Darmstadt, 2003
Polito, A.: Encefalopatia portosistemica in fase terminale in paziente cirrotico: terapia con SON Formula (MyAMINO®)
Purves, W. K. et al: Biologie, Spektrum Akademischer Verlag, 7. Aufl. 2006